Overview
 Morton?s Neuroma is a pain condition that affects your feet and toes. If you are suffering from Morton?s Neuroma, a growth of tissue has developed over one of the nerves running from your feet into your toes. This growth can cause inflammation and pain whenever you use your foot. A type of benign tumor, Morton?s Neuroma typically develops in the space between the third and fourth toes, although it can also form between the second and third toes. When you walk, the bones and ligaments in the top of your foot press down on this growth, causing pressure and pain.
Morton?s Neuroma is a pain condition that affects your feet and toes. If you are suffering from Morton?s Neuroma, a growth of tissue has developed over one of the nerves running from your feet into your toes. This growth can cause inflammation and pain whenever you use your foot. A type of benign tumor, Morton?s Neuroma typically develops in the space between the third and fourth toes, although it can also form between the second and third toes. When you walk, the bones and ligaments in the top of your foot press down on this growth, causing pressure and pain.
Causes
The exact cause is as yet unclear. However there are a number of theories. Some expert s believe problems with the design of the foot makes some people more prone to Morton?s neuroma. Having flat feet or a high arch for example encourages the foot to slide forwards which can put excess pressure on the metatarsals. Bunions and hammer toes also increase the likelihood of developing Morton?s. However simply wearing high heels or any form of tight shoes that put pressure on the bones in the feet can also lead to a Morton?s . Typically the condition comes on between the age of 40 and 50. It is far more common in women than men – three out of four sufferers are women.
Symptoms
People with Morton’s neuroma usually complain of pain that can start in the ball of the foot and shoot into the affected toes. However, some people just have toe pain. There may also be burning and tingling of the toes. The symptoms are usually felt up the sides of the space between two toes. For example, if the nerve between the third and fourth long bones (metatarsals) of the right foot is affected, the symptoms will usually be felt up the right-hand side of the fourth toe and up the left-hand side of the third toe. Some people describe the pain that they feel as being like walking on a stone or a marble. Symptoms can be made worse if you wear high-heeled shoes. The pain is relieved by taking your shoe off, resting your foot and massaging the area. You may also experience some numbness between the affected toes. Your affected toes may also appear to be spread apart, which doctors refer to as the ‘V sign’. The symptoms can vary and may come and go over a number of years. For example, some people may experience two attacks of pain in a week and then nothing for a year. Others may have regular and persistent (chronic) pain.
Diagnosis
You should visit a doctor or podiatrist (foot doctor) if you have pain or tingling that does not stop. Your health care provider will examine your feet and will apply pressure on the spaces between the bones of the toes to determine the location of the foot pain. The doctor may order X-rays to rule out other conditions associated with foot pain, such as a stress fracture or arthritis. X-rays alone will not show whether or not a neuroma is present, so an ultrasound scan or magnetic resonance imaging (MRI) test may be done to confirm the diagnosis. A diagnostic procedure called an electromyography is sometimes used to rule out nerve conditions that may cause symptoms like those of associated with Morton?s neuroma.
Non Surgical Treatment
There are various options for treating the condition, depending on its severity. Self-treatment. Here are some simple steps that may improve symptoms. Wear supportive shoes with a wide toe box. Do not lace the forefoot of the shoe too tightly. Shoes with shock-absorbent soles and proper insoles are recommended. Do not wear tight or pointed toed shoes or shoes with heels more than 2 inches high. Use over-the-counter shoe pads to relieve pressure. Apply an ice pack to the affected area to reduce pain and swelling. Rest your feet and massage the painful area. There are drugs that may temporarily relieve the pain and other symptoms of Morton?s neuroma. Long-term use of these medications is not recommended. Anti-inflammatory drugs-Nonsteroidal anti-inflammatory drugs, such as ibuprofen or aspirin, may be taken orally to reduce pain and inflammation. Anti-inflammatory drugs can also be administered by direct injection into the skin. Local anesthetic. An anesthetic injection will temporarily relieve pain by numbing the affected nerve. Orthotics. These are custom-designed shoe inserts that can reduce some of the pain associated with Morton?s neuroma. Sometimes padding is placed around the toe area, and tape is applied to hold the padding in place.
Surgical Treatment
If your pain continues despite several months of conservative treatment, your doctor may recommend surgery to remove the neuroma or to widen the space through which the affected nerve travels. These types of surgery often are done under local anesthesia. If your doctor removes a portion of the affected nerve along with the neuroma, you may develop permanent numbness between the toes.




 Overview
Overview Symptoms
Symptoms Prevention
Prevention



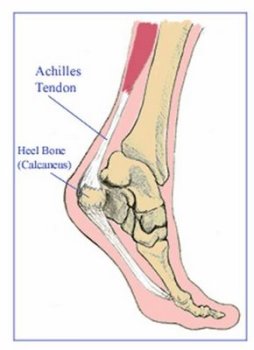
 Achilles tendinitis is very common among running athletes. The calf muscles attach to the calcaneus via the Achilles tendon. During running, the calf muscles help with the lift-off phase of gait. Repetitive forces from running combined with insufficient recovery time can initially cause inflammation in the tendon paratenon (fatty areolar tissue that surrounds the tendon). A complete tear of the Achilles tendon is a serious injury, usually resulting from sudden, forceful stress. Tendon tears can occur with minimal exertion in people who have taken fluoroquinolone antibiotics.
Achilles tendinitis is very common among running athletes. The calf muscles attach to the calcaneus via the Achilles tendon. During running, the calf muscles help with the lift-off phase of gait. Repetitive forces from running combined with insufficient recovery time can initially cause inflammation in the tendon paratenon (fatty areolar tissue that surrounds the tendon). A complete tear of the Achilles tendon is a serious injury, usually resulting from sudden, forceful stress. Tendon tears can occur with minimal exertion in people who have taken fluoroquinolone antibiotics.